Medicare cuts aren’t only going to affect payers in the MA space.
Medicare Advantage plans saw a final rate cut earlier this month, and it caused quite a stir amongst payers. A base rate cut of 0.16% will be seen in MA plans for 2025.
But ultimately payers will see an increase in MA payments in 2025 compared to 2024.
Overall the rate cut won’t bite off much from major payer businesses, but for others, it could.
Five other groups that will likely be more affected by the rate cuts are:
Smaller MA sponsors and their lobbying groups: these groups tried their best to defeat this rule and members will pay dues for the results.
Hospitals and physicians: these groups will see reimbursement cuts to care providers, especially smaller and rural health systems with large MA enrollment.
MA brokers, agents and marketing companies: these groups will see their profits affected by MA marketing tactic constraints as well as member transparency protections.
MA enrollees: this group will see fewer plan options and higher premiums.
Supplemental service providers: this group will see lower CMS payments and possibly be forced to reduce/eliminate supplemental benefits.
Will health insurers be prepared for a climate health crisis? They should be.
The climate crisis is longer confined to our TV set on National Geographic, it’s on our doorstep. From wildfires that choked the nation last year, to extreme heat that took lives, the notion that climate change is affecting our health is no longer an argument, it’s a reality.
For evidence of climate effects, look no further than last year, a.k.a the hottest year on record. Last year alone there were 28 climate disasters that cost the U.S. a whopping $92.9 billion.
Of course, not every storm, fire, and drought is caused by climate change. However, climate scientists state that a warming planet will increase the chances of more storms, more extreme heat waves, more droughts, and more wildfires. If that isn’t something that affects our health, what is?
What does that mean for the population? More health crises. What does that mean for health insurance? Skyrocketing utilization.
Climate Change and Health Insurance
Climate change is already affecting things like home insurance, making it more expensive and harder to obtain; health insurance is next in line.
A report by the Boston Consulting Group looked at how climate change will affect health insurance: “Beyond its impact on individuals, global warming puts a strain on health care providers, causes loss of work hours, and leads to higher economic costs. It is also leading to mounting claims and costs for health insurers.”
Beyond experiencing these disastrous climate events, climate-induced anxiety and depression also comes into play. From trauma and loss from these events to existential concerns about an unsteady future, the climate crisis is affecting our mental health too. This factor has the potential to raise utilization and expenses in mental and behavioral healthcare as well.
The CommonWealth Fund puts it as “further taxing a behavioral health care system already in crisis.”
What Does It Mean For Payers?
So how do health plans even begin to tackle such a problem?
One state that has experienced drastic climate effects, perhaps more than anywhere else in the country, is California; from fires, floods, and droughts to record heat—the state is no stranger to extreme weather.
HealthLeaders sat down with Baylis Beard, director of sustainability at Blue Shield of California, to hear their thoughts on climate change’s relationship with health insurance, its effect on healthcare, and what the organization is doing to prepare.
“We have seen our health systems get overwhelmed again and again – from Hurricane Katrina to Hurricane Maria and Sandy to the wildfires and flooding we see here in California,” Beard said.
Health plans are often less exposed to the frontline issues that clinicians face, but they are nonetheless responsible for providing sustainable care and providing resources to make the health system more resilient, Beard explained.
Beard also pointed out that healthcare isn’t entirely a victim in this problem. The US healthcare system contributes to 8.5 percent of U.S. emissions. In turn, climate change costs the healthcare system billions.
“And financially, pollution and climate change cost $820 billion in annual health care costs. Inaction will cost $8 trillion over 10 years according to the National Resources Defense Council,” Beard said.
Not Every Disaster Is Created Equal
While we can’t say we know for sure the effects climate change has on our health, we do know it affects some communities more than others. We can’t talk about climate change and solutions to it without at least acknowledging the disproportionate effect it has on minority groups. The health impacts of climate change are not felt equally.
The National Institute of Health explains that there is evidence of racial disparities in climate change regarding mortality, respiratory and cardiovascular disease, mental health, and heat-related illness. It also notes that children are particularly vulnerable, and infants of color have experienced poorer perinatal outcomes, heat stress, and higher emergency department visits in association with extreme weather.
According to The National Institute of Health: “The evidence strongly suggests climate change is an environmental injustice that is likely to exacerbate existing racial disparities across a broad range of health outcomes.”
“[...] We know that certain communities – particularly communities of color, the communities that contribute least to planetary harm – are the ones that already face disproportionate burdens of environmental pollution, and climate impacts on health,” Beard stated.
Looking Ahead
Health insurers are already well-positioned to tackle this problem; being able to predict, control for, and prevent risk is a philosophy health insurers know well.
In other parts of the insurance industry, like property and home insurance where climate change is already having an effect, these companies are reacting by pulling out of high-risk areas or limiting coverage, including in California, Beard explained. But this is not a sustainable solution.
“As the climate crisis continues to develop and exacerbate our big problems – cost, affordability, quality, access, equity and satisfaction – we must look at this as a catalyst for system transformation – for reimagining our healthcare system as a whole,” Beard said. “We can no longer accept the status quo.”
Now that you know why payers should care about climate change, check back for part two where we’ll dive into what payers can do about it.
Facing legal heat once again, Aetna just can’t seem to stay out of the spotlight. On April 16, a group of three Pennsylvania health systems sued Aetna for breaching the terms of their contract with Bridges Health Partners.
Aetna had been allegedly subtracting the cost from supplemental benefits such as meals and gym memberships from Centers for Medicare & Medicaid Services funds intended for patient care. In the contract, Aetna was supposed to reward Bridges with a share of the cost savings that were below a specific medical cost target, then they were to provide additional payments for meeting agreed upon quality metrics, according to a press release.
However, Aetna did not pay what was due and instead stacked up the supplemental benefit costs that included gift cards and over-the-counter medications, which were only available through Aetna’s parent company CVS, therefore directing millions of dollars towards CVS and charging the cost back to Bridge providers.
Bridges alleges that Aetna was funneling money back to parent company CVS and called the supplemental programs "marketing expenses" designed to attract more members.
Bridges also stated in the press release that the health system is losing millions of dollars that it earned in shared savings, which is impacting the financial wellbeing of Bridges’ providers.
Dr. Robert Zimmerman, Bridges Health Partners president and chief medical officer said in the press release: “While the incentives are good programs, they are not critical care health programs. They are supplemental programs that potentially erode a patient’s care at our providers. If we have to pay for the incentives, we cannot provide cost-saving, patient-centered care. It’s egregious manipulation but also a breach of our contract with Aetna.”
Bridges Health Partners requested that a judge issue an injunction that would require Aetna to abide by the terms of its contract as well as reimbursement of funds and legal fees.
“Health plan organizations, like Aetna, are setting record profits while community-based hospitals and health systems are struggling. This is a national crisis,” John Grese, Bridges Health Partners vice president of administration, said in the press release. “If the insurance agency corporate giants are not stopped, community health care will be obsolete, putting thousands of doctors, nurses, and staff out of jobs and the very people needing treatment will be the ones who suffer. “
Last year, Aetna’s peak revenue was $60.6 billion, roughly about $1.3 million to each employee out of 47, 950 employees.
This isn’t the first time Aetna has geared up for a lawsuit. Last year, the insurance giant saw 21 lawsuits in just one week. A New Jersey federal court accused Aetna of failing to fund reconstructive surgery for breast cancer patients who’ve had mastectomies.
Aetna was also hit with a different lawsuit last month for allegedly discriminating against non-heterosexual patients through its coverage of fertility treatments. The case moved forward after a federal judge dismissed one of the lawsuit’s three claims.
An audit by the U.S. Department of Health and Human Services' Office of the Inspector General from last year also found that Aetna received an estimated $25.5 million in Medicare Advantage overpayments for 2015 and 2016.
This case with Bridges Health Partners could have the potential to reshape Medicare Advantage supplemental benefits. The case could prompt insurers to possibly do away with coverage of benefits such as gym memberships and over-the-counter medications.
Another possible outcome could be Aetna facing a bumpy road to securing future provider contracts. As the cases (and new coverages) pile up, health systems are surely aware of Aetna’s alleged dishonest practices. The consistent court cases could potentially shine a softer light on other insurers when it comes to contract renewals. As Aetna gets battered in court, other payers should take note of the legal repercussions when they breach the terms of their contracts; providers and health systems have no interest in working with manipulative partners.
U.S. health system spending on social determinants of health could jump even higher.
Health systems are struggling to find a strategy to identify and address social determinants of health.
A study by Deloitte shows that in the U.S. health inequities cost the healthcare industry roughly $320 billion every year. By 2040 that could jump to $1 trillion if the industry fails to take action.
To address this, health systems would have to understand why they spend thousands of dollars more each year to treat minorities for the same chronic conditions seen in white patients.
Check out the accompanying article and a new AI based tool that may be able to help here.
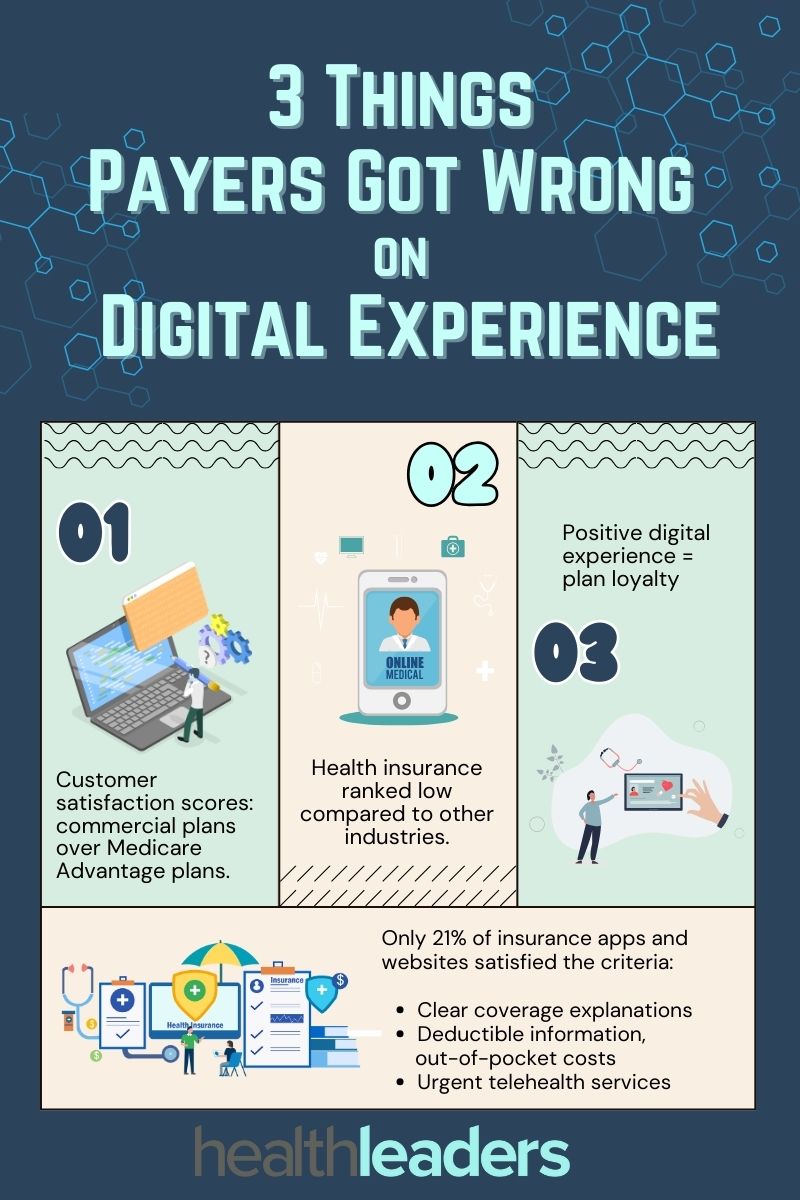
Digital experiences in healthcare have progressed exponentially over the last few years: from administrative AI to smartphone app diagnosis, but payers seem to have fallen behind in this realm. According to a J.D. Power report, the digital insurance experience isn’t where it should be.
J.D. Power defines four basic functions of apps and websites, including: digital functionality, organization and visual appeal. Out of the 5,590 members that were surveyed, including the 14 largest Medicare Advantage plans and 15 of the largest commercial member health plans, roughly one third of insurer’s apps and websites failed on these basic functions.
Overall only 21% of the digital properties met all the criteria to be considered high-functioning digital solutions, such as clear explanations of coverage, provided information on deductibles and out-of-pocket costs, and offering urgent telehealth services.
Here are three notes on the digital insurance experience:
Commercial plan members had a better digital experience than MA plan members, and overall rated it more highly: commercial plan apps and websites had an average customer satisfaction rating 646 out of 1,000, compared to 629 for MA plans.
Health insurers ranked low for digital experience compared to other industry scores. Property and casualty insurance averaged a score of 700 for customer satisfaction, and self-directed wealth management apps had a score of 718.
When MA plan members had a positive digital experience, it was linked with their intent to stay with the plan. In MA plans that received scores of 801 or higher, 89% of members said they would definitely stick with the same plan.
Medicaid unwinding left millions uninsured, particularly children, Black, Hispanic and lower income communities.
Roughly one quarter of Americans who were disenrolled from their pre-pandemic Medicaid coverage are now completely uninsured. Why? High costs and other procedural hurdles that particularly affect minorities and lower income communities who rely heavily on federally funded coverage. Plainly, health coverage is too expensive and trying to prove eligibility can sometimes feel like a fool’s errand.
The provision that kept states from disenrolling consumers from Medicaid during the COVID-19 pandemic ended in March 2023. The Biden administration projected about 15 million people would lose their coverage, but 20 million did instead, according to a Kaiser Family Foundation report. Most states will have until June to continue conducting eligibility reviews, and that 20 million is expected to grow.
The Fight for Coverage
The biggest hurdle for acquiring coverage for more than half (54%) of uninsured adults is simply cost. KFF’s survey looked at over 1,200 adults in February and March 2024, including individuals who stated they had Medicaid coverage in early 2023, prior to the ending of pandemic eligibility rules in April 2023.
Two-thirds (64%) of individuals who were enrolled in Medicaid before the unwinding process began say they took action in 2023 to renew their coverage. The survey found that about one-fifth of all individuals who had Medicaid coverage in early 2023 were disenrolled sometime later that year. Over one-third who attempted to regain any type of coverage said the process was difficult, and about half (48%) called it stressful.
Long call center wait times, excessive paperwork and uncertainty about what paperwork was needed were common complaints. Some states that have not expanded Medicaid require proof of residency in order to renew coverage, creating yet another hurdle. The survey shows that individuals living in non-expansion states were at least twenty percentage points more likely to say they were asked to submit proof of residency. If the state is unable to obtain eligibility documents electronically, then they may put the task back on the enrollee to submit these documents.
Additionally, Black and Hispanic groups were much more likely than White groups to say they were asked to submit proof of residency to regain coverage: Black groups (71%), Hispanic groups (60%), and White groups (42%).
A recent KFF tracking poll also found that seven out of ten of the overall public (69%) said they heard only “a little” or “nothing at all” surrounding state removals of enrollees from Medicaid as pandemic provisions came to an end.
The survey showed that groups with lower levels of education, particularly those with a high school diploma or less, were far more likely to say they heard “nothing at all” about states removing enrollees from Medicaid.
Apart from administration processing issues and procedural hurdles on Medicaid’s end, among those who took action to renew their coverage, about 14% said they did not have reliable internet access to complete the forms online.
The survey also shows the clear and immediate impact of loss of coverage on health: over half (56%) of individuals surveyed said they missed a necessary healthcare appointment or skipped their prescriptions as they waited to regain coverage.
Who’s Most Affected?
Medicaid enrollment jumped by almost one-third during the pandemic, from 71 million in February 2020 to 94 million in April 2023. But this data isn’t complete, as it doesn’t reflect one of the largest groups affected by Medicaid coverage loss: children.
Children have the highest official poverty rates of any age group. In 2022 about 16% of children aged 0-18 were living in poverty, according to a KFF news report. Furthermore, the report states that in 2022 supplemental poverty rates were the highest for asian children (25.9%), hispanic children (19.5%), and black children (17.8%).
KFF news released a report on April 15 that showed in Texas two million consumers were disenrolled from Medicaid in March 2024, and 1.34 million of those individuals were, you guessed it, children.
The Fix
Overall, those still on Medicaid rate the program positively across all groups. The survey shows that ratings are also consistently positive in both expansion and non-expansion states. Individuals are happy with Medicaid coverage, all things considered. The issue is in acquisition.
As of now, roughly 30 million individuals are still awaiting Medicaid renewals.
Is there room for payers to intervene here? With millions losing coverage, is there any opportunity for payers to put forth new plans or aid in offering affordable supplemental coverage that targets these groups? Maybe, but not without federal allyship, and not without reexamination of this important federally funded coverage, and the procedural barriers that accommodate it.
Payers and providers shouldn't underestimate the value of streamlined, accurate data, especially when it comes to contract negotiations.
HealthLeaders sat down with Britt Barrett, managing director and teaching professor at Brigham Young University and former CEO with HCA, Texas Health Resources, and SHARP, to discuss what needs to be done in order for data to be leveraged for both payers and providers in contract negotiations.
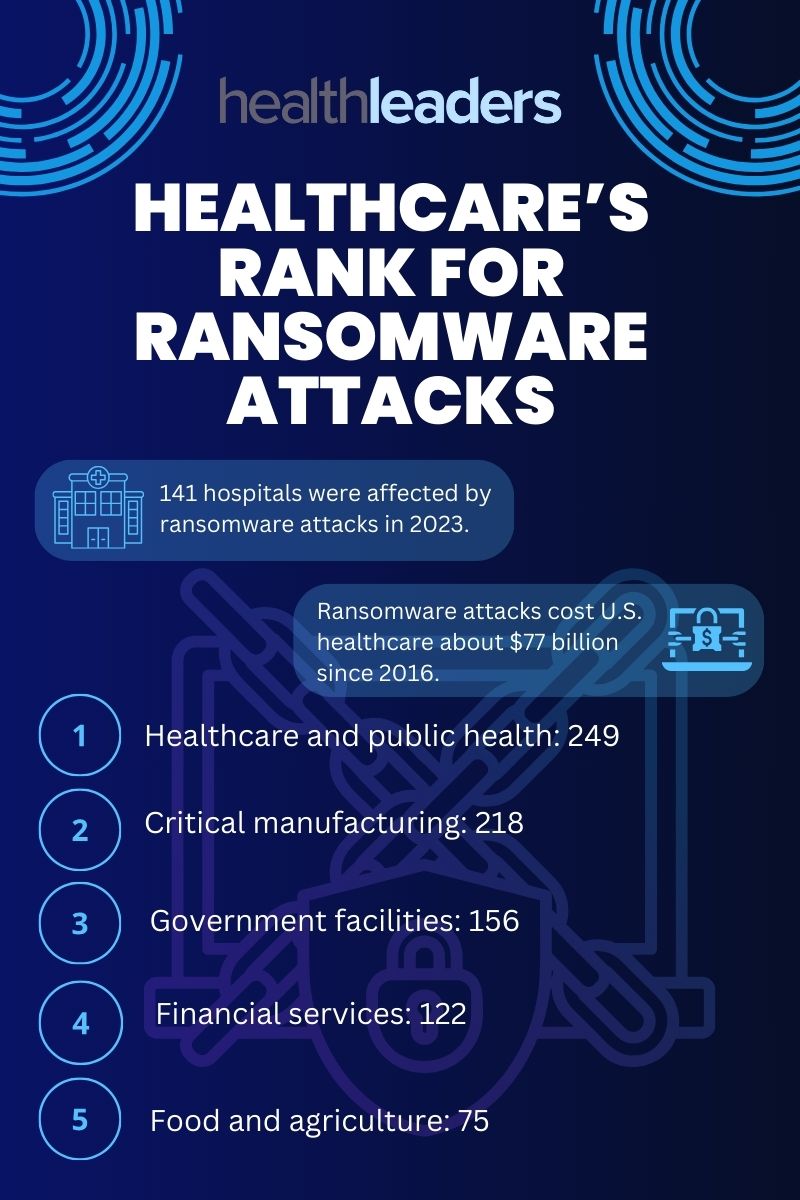
Healthcare has a big target on its back when it comes to ransomware attacks.
Ransomware attacks affect dozens of different sectors, but healthcare seems to be a particular favorite. An analysis published by EmsiSoft looked at just how big the ransomware problem is for hospitals and health systems.
Firstly, ransomware attacks are difficult to gather data on because many of them aren’t recognized as ransomware attacks. “Encryption events” is a term often used which can make tracking these events a challenge, reported cybersecurity firm Emsisoft.
In 2023 over 2,000 hospitals, schools and governments were directly impacted by ransomware attacks. The Change Healthcare attack is just the latest in the mix, and now they may even be facing another one.
At least 141 hospitals were affected by ransomware attacks last year, and cost U.S. healthcare organizations about $77 billion in downtime alone since 2016.
So far, despite government task forces, asset seizures and arrests have been implemented, but ransomware attacks persist. One solution may even be to outright ban the payment of ransoms, according to Emsisoft, stating in a blog post: “If it is made unprofitable, most attacks will quickly stop.”
The massive issue is only set to worsen unless health tech experts can find viable solutions to protect health systems from these attacks. Check out this infographic for a breakdown of where healthcare falls in ransomware attacks.
Medicare Advantage has gone through numerous changes and hurdles since its creation.
The recent rate cut to Medicare Advantage is the biggest change we’ve seen to the program since 1997. Created over thirty years ago, Medicare Advantage has gone through much evolution, ups and downs of popularity, and regulation pressures since it began. With the original intention of giving consumers a Medicare option beyond the traditional fee-for-service program, and bringing the financial savings and efficiencies in managed care in the private sector, MA has become a public favorite in recent years with higher utilization.
MA has generally been more expensive than Traditional Medicare, and those overpayments have increased in recent years. In 2019 MA spending was up an estimated $7 billion compared to Traditional Medicare.
The recent rate cut to MA signals a significant shift in the program that has been a public favorite in recent years. For the payer, this change could impact business by potentially reducing overpayments and increasing competition within the MA market.
It is important for payer c-suite leaders to closely monitor these developments and adjust strategies accordingly to remain competitive in the evolving landscape.
Take a look at how MA has changed over time since its creation.
Medicare Advantage Timeline
1982: Tax Equity and Fiscal Responsibility Act (TEFRA) authorizes Medicare to contract with risk-based private health plans.
1985: Rules to implement risk-based contracting are completed and Medicare Part C begins.
1997: Balanced Budget Act: program renamed to Medicare + Choice: Medicare payments are reformed by extending per-case payment methods to all categories of post-acute care.
2000: Benefits Improvement and Protection Act (BIPA) restores approximately $11.5 billion over five years to hospitals under Medicare, Medicaid, and other federal and state health care programs, but fails to reverse the declining participation of Medicare plans and the enrollment of beneficiaries.
2003: Medicare Modernization Act: Name changed to Medicare Advantage.
2010: Reductions in MA payments are made by Patient Protection and Affordable Care Act.
The new rate cut will have a strong impact, but not on big payers.
Just about every insurer is up in arms over the new Medicare Advantage rate cuts.
To recap: MA plans will see a base rate cut of 0.16% in 2025 since risk scores are expected to be 3.86%. The expected average change in revenue will be 3.7%, and CMS notes that “this is an increase of over $16 billion in 2025 compared to 2024 in expected MA payments.”
However, this rate cut isn’t going to be a huge blow to big payers. Yes, we saw their stocks take a dive when it was announced, but it won’t be detrimental to their business.
MA insurers started the 2023 year financially stable, even considering the uptick in utilization late in the year. The giants still showed strong profits in the billions: Humana at $2.5 billion, Cigna at $5.2 billion, UnitedHealth at $22.4 billion, Elevance at $6 billion, Centene at $2.7 billion, CVS (Aetna) at $8.3 billion…you get the picture.
The rate cut is still a big deal. It's the biggest change in Medicare since Medicare Choice was included in the Balanced Budget Act of 1997, which reformed Medicare payments by extending per-case payment methods to all categories of post-acute care.
Pressure for small insurers
It will be a bigger deal for smaller insurers. Industry expert Paul Keckley dives into who will be most affected by this MA change in his Keckley Report. A few groups he says will feel the brunt of the change are:
Smaller Medicare Advantage sponsors and their lobbying groups will take a hit after trying their best to defeat this rule and members will pay dues for the results.
Hospitals and physicians will feel the effect of this rule in the form of reimbursement cuts to care providers, especially smaller and rural health systems with large MA enrollment.
MA brokers, agents and marketing companies may feel a hit to their profits from constraints of MA marketing tactics and member transparency protections. These could reduce revenue for third-party marketing organizations that sell their services to these plans. Keckley says that a shakeout is likely.
MA enrollees may see fewer plan options and higher premiums, thickening the barrier to access affordable healthcare. Although the ruling adds benefits for behavioral health and data privacy protections, it most likely won’t outweigh the stiffening premiums and fewer plan options. Keckley says that while big MA plans will be hurt but will adapt, while small plans will be left in the dust.
Supplemental service providers will see lower payments from CMS and may be forced to reduce or eliminate supplemental benefits that aren’t as important to members. Keckley surmises that benefits like fitness programs may be cut, but dental and prescription drug benefits appear to be safe.
Lastly, the 2024 Presidential campaign is happening right alongside this MA change and Keckley says that he has no doubt the campaigns “will opine to Medicare security in their closing rhetoric recognizing MA covers more than half its enrollees.” MA insurers will submit their new plans to CMS by June 3 and open enrollment begins in October, a month before the nation votes for the next president.
Overall, this MA rule will affect all plans in one way or another, whether it’s day to day operations, heightening friction with providers or reimbursement negotiations, Keckley concludes in his report that MA is simply a work in progress.







77df.jpg)
46fc.jpg)
9d79.jpg)
2679.jpg)
c3da.jpg)