HealthLeaders offers a look at issues and trends that are shaping the business of healthcare in the United States today. Free to download.
High-Cost Commercial Claimants
September 2017
The American Health Policy Institute (AHPI)1 defines high-cost claimants (HCC) as those patients who cost $50,000 per year. In a 2016 study of 26 large employers, AHPI found that HCCs cost an average of $122,382 annually, and that they comprised 31% of total spending. Both payers and providers are concerned about the etiology behind the cost of care for these patients.
Payers are putting pressure on providers to take on greater risk and mitigate cost as they move to value-based care and better outcomes. Payers faced with increasing healthcare costs are looking to consumers to become more engaged from both a financial and care perspective.
Hospitals and payers are focused on preventing and reducing the health and cost consequences of the adverse events so starkly highlighted by the Institute of Medicine’s 1999 seminal report on patient safety, To Err Is Human.
Adverse events are defined as either the failure of a planned action to be completed as intended, or the use of a wrong plan to achieve an aim. In 1999, the total cost of these events, including indirect costs, was estimated to be as high as $29 billion a year. In the United States, patient safety continues to be a priority, as part of a drive toward value. Patient safety events can directly impact hospital revenue. CMS’ Hospital-Acquired Condition Reduction Program penalizes reimbursements by 1% for hospitals achieving the bottom quartile in performance scoring.
This study presents the incremental consequences of selected inpatient medical injuries as identified by the Agency for Healthcare Research and Quality (AHRQ) Patient Safety Indicators (in terms of mortality, length of stay, and total hospital cost per case among national U.S. inpatients), and quantifies the estimated overall impact of such events at the national level.
With premiums on the rise and commercial payers interested in increasing the value return on their healthcare investment, more payers are considering value-based care arrangements.
While CMS has led the charge to use bundled payments for joint replacements through the Bundled Payments for Care Improvement (BPCI) and Comprehensive Care for Joint Replacement (CJR) program, there is increasing interest in these arrangements from the payer market.
As payers and providers begin to anticipate and plan for the change,it’s important to study bundled payments from a variety of angles looking at cost variations by region, market, provider type, and payers.
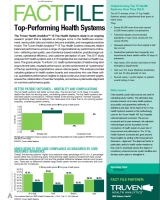
The Truven Health Analytics™ 15 Top Health Systems study is an ongoing research project that is adjusted as changes occur in the healthcare environment, newly public data and metrics become available, and managerial practices evolve.
The Truven Health Analytics™ 15 Top Health Systems measures relative balanced performance across a range of organizational key performance indicators— reflecting care quality, use of evidence-based medicine, postdischarge outcomes, operational efficiency, and customer perception of care. This analysis provides valuable guidance to health system boards and executives who use these critical, quantitative performance insights to adjust continuous improvement targets,ensure the collaboration of member hospitals, and achieve systemwide alignment on common performance goals.