The core elements of promoting quality care include three things, says this CMO.
Quality care is going to be a primary focus of the new CMO of Lifepoint Health.
Last month, Chris Frost, MD, was named senior vice president, chief medical officer, and chief quality officer of Lifepoint. He has served in two other leadership roles at the Brentwood, Tennessee-based health system: chief medical officer of Lifepoint Communities and national medical director of hospital-based services.
Frost says the core elements of promoting quality care include three things: a leadership component, a process improvement component, and a culture of safety.
"Those are the framework components of our Lifepoint National Quality Program," Frost says.
The leadership component includes the recognition of the importance of leadership in every aspect of the organization, according to Frost. It also includes engagement of all the quality stakeholders and an accountability process.
For process improvement, he says Lifepoint has a checklist of ten critical components for performance improvement such as huddles that clinical care teams use to focus on clinical workflows, learning whiteboards at every clinical care unit to identify opportunities for improvement, and tracking data that demonstrates progress or regress.
The culture of safety at Lifepoint includes the engagement of patients and their families as well as fostering an environment where all team members experience psychological safety and have a voice in the safety process, according to Frost.
Frost says the Lifepoint National Quality Program, which started in 2010 and is a combination of both quantitative and qualitative criteria, will be one of his main areas of attention.
"We have a deliberate focus on reduction of patient harms such as catheter-associated urinary tract infections and central line-associated bloodstream infections," Frost says. "We have demonstrated significant progress since starting the national quality program, including a 65% reduction in our overall patient harms."
Lifepoint has also recognized that there are external barometers of patient safety and quality of care such as The Leapfrog Group and Centers for Medicare & Medicaid Services Star Ratings, according to Frost.
"We have deliberately focused on integrating components of Leapfrog and CMS Stars into our national quality program," Frost says. "The point is that quality and the definition of quality have tried and true components that you see year-over-year, but it is not a static process. It is a dynamic process that requires evolution."
Chris Frost, MD, is senior vice president, chief medical officer, and chief quality officer at Lifepoint Health. Photo courtesy of Lifepoint Health.
Engaging a clinical staff
There are four facets of clinical staff engagement, according to Frost.
First, a CMO must make a deliberate effort to deconstruct historically hierarchical models of care, says Frost, who adds physicians have had an outsized influence in healthcare in the past.
"One of the success measures for engaging clinical staff is making sure that the definition of clinical staff is not limited to physicians," Frost says. "It includes physicians, advanced practice providers, nurses, physical therapists, pharmacists, and other clinical professionals."
Second, a CMO must leverage data and analytics, according to Frost.
"Data and analytics are related to the mantra of 'that which can be measured can be managed,'" Frost says. "Analytics allow us to convert raw data into a clinically meaningful narrative—how data demonstrates how our clinical workflows impact our patients."
Third, a CMO must manage quality-focused process improvement, according to Frost.
"You want to use a plan, do, study, act (PDSA) cycle," Frost says.
Fourth, a CMO must engage in change management, according to Frost.
"For process improvement to take root and to be sustained, you must have clinicians and staff willing to do things differently," Frost says. "Change management is the people side of change."
Prepared to lead
Frost says his clinical background in internal medicine and pediatrics provides a solid foundation for working in the CMO role.
Combined internal medicine and pediatrics training is usually a four-year program. Physicians do two years of internal medicine training and two years of pediatrics training, then they are eligible to become board certified in both specialties.
"The training allowed me to understand the social and clinical needs of the patient population from cradle to grave," Frost says.
Frost served as a hospitalist for nearly two decades, and he says his hospital medicine background is also beneficial in his new role.
"That experience has been incredibly helpful for the CMO role because I have an intimate understanding of the continuum of care of the patients," Frost says, "from the ambulatory setting to the acute care setting, to the post-acute care setting."
Challenge in Lifepoint markets
A key challenge at Lifepoint is serving nonurban communities, according to Frost.
"One aspect of Lifepoint's mission to make our communities healthier is allowing community members in nonurban settings to access care close to home," Frost says. "The challenge here includes physician recruitment and nurse recruitment."
To address these challenges, Lifepoint has been leveraging telehealth as a way to have critical clinical services offered to nonurban community members, according to Frost, who adds the health system has established nurse residency programs as a way to help train and introduce nursing team members to nonurban communities.
Another important aspect of serving patients in nonurban communities is addressing social determinants of health, according to Frost.
"We have seized on partnership opportunities with community organizations to address social determinants of health," Frost says. "This includes food insecurity, housing insecurity, and interpersonal safety. The health system is not necessarily positioned to address all social determinants of health, but partnerships with our community organizations have been meaningful work for our team members."
Allegheny Health Network has generated positive results from its physician well-being efforts, with physician burnout rates running at about 10% below the national rate.
The best physician well-being programs begin by measuring burnout and well-being, then selecting an appropriate strategy, the chief wellness officer of Allegheny Health Network (AHN) says.
Burnout takes a personal and professional toll on physicians, says Thomas Campbell, MD, MPH, chief wellness officer at AHN.
"On the personal side, there is increased substance abuse," he says. "Studies have shown that alcohol use and other substance use increases with higher levels of burnout. There is trouble with relationships at home with loved ones. There is also an increase in suicidal ideation and depression."
"On the professional side, increases in physician burnout cause decreases in quality of care, which we see with increased malpractice claims and increased near misses in patient safety events," he says. "There is a decrease in productivity—the efficiency of physicians and their ability to see more patients is decreased. Finally, burnout causes physicians to cut back hours or to leave the profession."
AHN launched a wellness program for physicians, advanced practice providers, nurses, and residents six years ago. The first step was to measure burnout and well-being, Campbell says.
"One of the reasons we use a measurement tool regularly is we didn't want to just try interventions and see how they worked," he says. "We want to have information from our survey that we can act on to pick interventions."
AHN selected a survey tool developed by a company at Penn State Health.
"We looked for a measurement tool that had validity for physicians, advanced practice providers, nurses, and residents," Campbell says. "They had experience measuring well-being and burnout for all those categories of workers, not just physicians. The company was led by a psychologist named Dan Shapiro, and we have continued to work with him over the past six years."
"They used Maslow's Hierarchy of Needs adapted to a healthcare industry well-being model, which includes basics such as good hydration and nutrition, moving up the pyramid to camaraderie, safety, appreciation, and feeling that you are contributing at full capacity," Campbell says.
The survey data indicates that AHN's well-being and burnout program is having a positive effect. Physician burnout levels have been running at about 10% lower than the national rate.
Thomas Campbell, MD, MPH, is chief wellness officer at AHN. Photo courtesy of AHN.
Setting a strategy
After selecting a measurement tool, AHN picked an established strategy for its wellness program. The health system picked the Stanford Model of Professional Fulfillment, which features three pillars: culture of wellness, efficiency of practice, and personal resilience.
1. Culture of wellness
The first step involves making sure that providers have multiple ways to reach out for help, Campbell says.
Survey data showed that physicians are reluctant to reach out to AHN's employee assistance program (EAP) because they are concerned about confidentiality.
"We created a help line so physicians could reach out to internal behavioral health providers 24/7," Campbell says. "We now have an EAP program that does not use internal reporting tools if people are uncomfortable with our internal behavioral health resources. We also established external resources, where people could get help through our county medical society."
AHN also conducted leadership education to create a culture that included psychological safety, so that physicians could feel comfortable sitting down one-on-one with their leaders, according to Campbell.
"The primary focus of the leadership training was how to lead your physicians with wellness in mind," he says.
The health system also removed questions about mental health history on physician credentialling forms.
"Those questions are a hinderance because they stigmatize doctors and prompt them to not reach out for help," Campbell says.
2. Efficiency of practice
Efficiency of practice is an essential element of promoting physician well-being, Campbell says.
"When you have a workday where everything is working well, you are less likely to get burned out," he says. "You are likely to get out of work on time, to be more fulfilled in your day, and to make yourself a better person physically and mentally outside of work."
AHN's effort to improve efficiency has focused on their Epic electronic health record.
"We have been trying to limit the amount of time physicians are on a computer to make their work more patient-centered," Campbell says. "We want physicians to spend less time at night—we call it pajama time—charting because they could not get to it during the workday."
To address this, AHN has formed teams of proficient Epic users to help physicians use the EHR more effectively.
"We call members of these teams IT officers, and these officers show physicians how to be more efficient in the EHR," Campbell says.
The health system has also adopted AI-driven ambient listening technology, which automates documentation during physician encounters with patients.
"We are trying to find ways to make the EHR work for the physician to promote a more efficient workday, create better documentation, and create tools that support better care," Campbell says.
AHN has also been working to build better teams around physicians
"We have been looking at what advanced practice providers, experienced nurses, and medical assistants can do together with physicians to create an optimum team working at the top of their capacity," Campbell says. "We are trying to establish more synergy and efficiency in the practice of medicine."
This team building effort has been particularly successful, he says, in the outpatient setting.
"In outpatient clinics, there is a great opportunity to allow advanced practice providers to do more within the scope of their licensure," Campbell says. "In the outpatient setting, we are also getting more out of nurses and nurse navigators."
3. Personal resilience
For physicians, teamwork is also tied to personal resilience and a commitment to wellness, Campbell says.
"We have found that resiliency is tied to the team around physicians, but physicians do need to keep an eye on their health and well-being," he says.
It is important to understand that personal resilience is individualized, Campbell says.
"What one person might need in terms of diet, sleep, hydration, and mental healthcare is often different than what another person might need to keep healthy," he says.
Campbell has found that his human resources colleagues and AHN's benefits offerings are crucial to supporting personal resilience.
"I have been looking at what programs that we have and what benefits that we have for those who may need help with issues such as weight management and addiction, including smoking cessation," he says. "We want to provide multiple ways for people to get the things that they need."
One such benefit is paternity leave and maternity leave, the latter of which was recently expanded.
An important element of personal resilience is finding ways to balance work and life outside of work, Campbell says.
"It is hard to achieve a perfect balance and a better term is probably integration," he says. "We have encouraged physicians to look at the integration of their work life and their personal life."
A national concern
The most recent survey data from the American Medical Association shows physician burnout below 50% for the first time since 2020. In 2023, 48% of physicians reported experiencing at least one symptom of burnout, which was down from 53% in 2022, according to the AMA. Physician burnout reached a record high in 2021, with 62% of physicians reporting at least one symptom of burnout, AMA survey data found.
Despite the improvement, physician burnout remains a troubling problem, according to the AMA.
"The shift marks a milestone in the ongoing battle against physician burnout, but the fight is far from over," a prepared statement from the AMA says. "Continued efforts are essential to address the root causes of physician burnout and ensure that doctors receive the support they need to thrive."
Campbell recently led a HealthLeaders strategy call on physician well-being.
Ashish Patel plans to translate his success in growing Phoenix Children's gastroenterology program into the physician-in-chief role.
The new physician-in-chief of Phoenix Children's earned the role based on his performance as division chief of gastroenterology at the pediatric health system.
Ashish Patel, MD, became division chief of gastroenterology at Phoenix Children's in April 2020. His prior leadership experience includes serving as associate clinical director of the pediatric gastroenterology program at University of Texas Southwestern Medical Center and director of the Southwestern Pediatric Inflammatory Bowel Disease Center at Children's Medical Center Dallas.
As division chief of gastroenterology, Patel says he pursued a program of excellence based on three pillars: clinical excellence, opportunities for research, and education and community outreach.
Clinical excellence
Patel promoted clinical excellence in the gastroenterology division by recruiting several new physicians. They were needed because of massive growth in the Phoenix area and growth of the health system.
"With a commitment to growth, the first thing we needed to do was to build on Phoenix Children's clinical excellence, and the way you do that is through recruiting excellent physicians," he says.
Patel recruited 10 new pediatric gastroenterologists, increasing the number of faculty positions in that area to 25. He also recruited two transplant-trained hepatologists and a pediatrics-trained liver and kidney surgeon.
In addition to addressing growth in the patient population, Patel's recruitment of new physicians was designed to fill gaps in the kind of care that Phoenix Children's provided. For example, there was no gastrointestinal motility program at the health system and there were no facilities in the state providing that service.
"We had to send patients to Texas to get motility studies done," Patel says. "I recruited a doctor from UT Southwestern to set up the motility program. He was among my first set of recruits. That allowed us to establish that we were in a growth phase, and people across the country saw that, which helped to boost recruitment."
There is a physician shortage in many specialties in the United States, but Patel was able to recruit physicians by leveraging his relationships and the growth opportunities at Phoenix Children's.
"One of the doctors we recruited was my first pediatric resident at UT Southwestern," he says. "Another doctor we recruited was one of my fellows at UT Southwestern. I talked with doctors about the vision and the opportunity at Phoenix Children's."
Ashish Patel, MD, is physician-in-chief of Phoenix Children's. Photo courtesy of Phoenix Children's.
Opportunities for Research
Patel says he learned the value of research at healthcare organizations from his time at UT Southwestern, an institution steeped in research.
"When I came to Phoenix Children's, I knew that the way we could build a national reputation was by being involved in research and being involved in efforts such as consortiums and collaborations," he says.
In 2020, research at Phoenix Children's was limited to a handful of industry-based studies that brought novel therapeutics to the pediatric population.
"What we wanted to do is add investigator-initiated studies that would advance science, medicine, and therapeutics," Patel says. "We have launched these kinds of studies in areas such as inflammatory bowel disease and feeding disorders."
An innovative area of research at Phoenix Children's is transnasal endoscopy, which does not require general anesthesia. Phoenix Children's and Children's Hospital of Philadelphia are national leaders in pediatric transnasal endoscopy.
"Transnasal endoscopy has benefits for children because they can avoid general anesthesia," Patel says. "It has benefits for the healthcare system in off-loading surgical caseload."
Education and community outreach
In 2020, Phoenix Children's had the largest pediatric gastroenterology program in the country that did not train future gastroenterologists. Creating a fellowship program was among Patel's top priorities, and a program was launched in 2021.
The goal was to create one of the best pediatric gastroenterology fellowship programs in the country, Patel says.
"When the core group sat down to plan for the fellowship program, we talked about what we loved about our fellowship experiences and what we thought could be done better," he says. "We wanted to achieve the perfect intersection of those things."
In the first year of interviewing fellows, candidates were told that the program offered an excellent clinical foundation, with opportunities for research, Patel says.
"Fellows would leave the program feeling comfortable in taking care of pediatric gastroenterology patients in multiple subspecialties," he says. "We also wanted to give fellows experiences in research—curriculum development, basic science research, clinical research, and quality improvement."
The gastroenterology fellowship program has been a success, Patel says.
"We have matched with fellows in each of the three years that the program has been open," he says. "In the past year, we recruited two fellows from our own residency program."
Since 2020, Phoenix Children's has launched several gastroenterology community outreach programs.
"Phoenix Children's foundation does amazing outreach throughout the Phoenix area," Patel says. "We have piggybacked on their resources to go out into the community to engage with families. We have created a Gastrointestinal Advisory Board, where we have asked families to advocate for what they feel is important in the GI field."
For example, this month an inflammatory bowel disease support group will meet at Phoenix Children's, Patel says.
"We will have an evening event where families can get some education, exposure to the research we are doing, and exposure to the support services that we have for our patients," he says.
Applying division chief success in the physician-in-chief role
Patel is eager to translate his division chief success to his new role.
"Now, my job is to take what I learned in growing the gastroenterology division over the past four years and take the approach of developing a vision, emphasizing mentorship and education, and promoting research at the 20 medical divisions at Phoenix Children's," he says. "I am going to be interacting with colleagues at the division-chief level."
Patel also plans to interact with the clinical staff.
"I want to attend their monthly faculty meetings, and I want to find out about their struggles," he says.
Two areas on which he focused as chief of gastroenterology are going to be particularly helpful in the physician-in-chief role, Patel says.
"I want to talk with the division chiefs about faculty outreach and recruiting," he says. "I want to help engage physicians and optimize recruiting."
Locum tenens clinicians can be a short-term solution for doctor shortages, but CMOs must plan carefully how to use them.
Locum tenens physicians can plug short-term gaps in the physician workforce, but CMOs must be aware of both the cost and the effect on workplace culture.
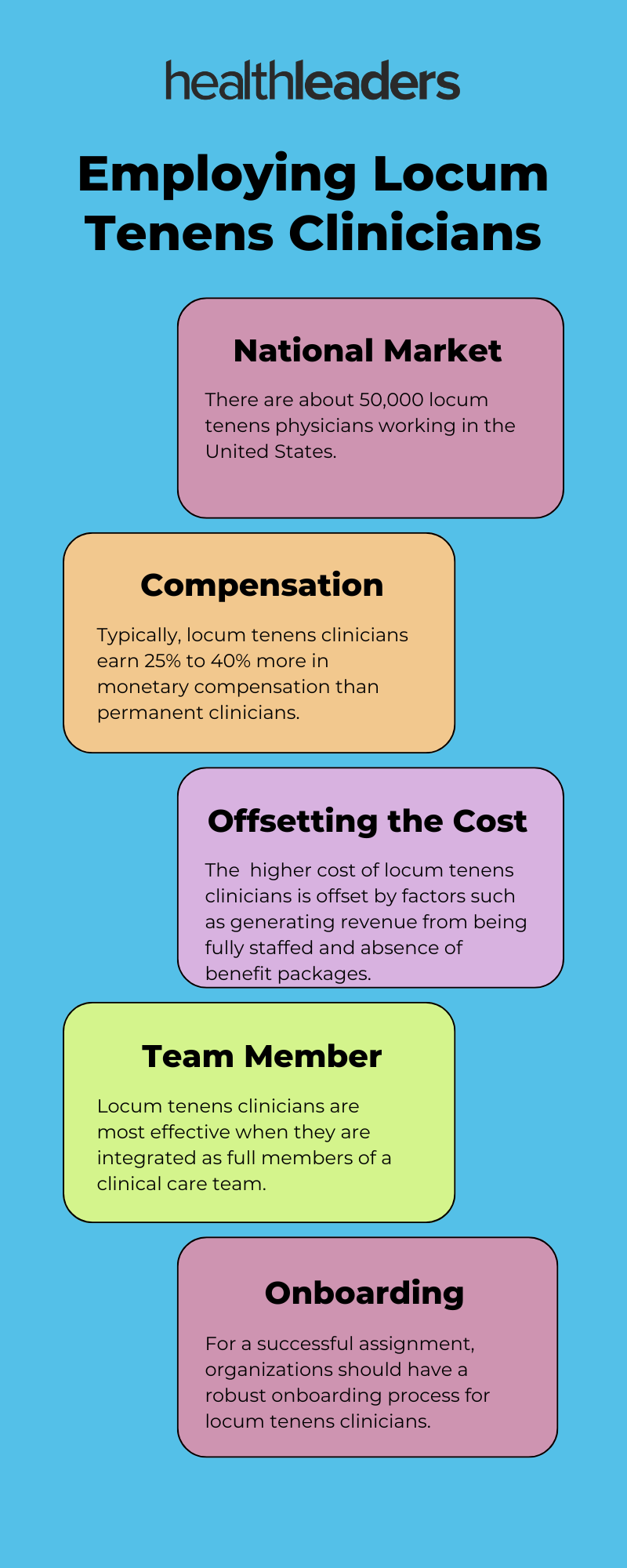
There are about 50,000 locum tenens physicians working in the United States, says Joseph Sturdivant, MD, CMO of IMN Enterprises, a healthcare staffing company. With a clinician shortage nationwide, he notes, they're a popular solution to fill workforce gaps.
About 88% of the nation’s health systems used locum tenens clinicians in 2023, Sturdivant says, and half of them expect to use more in 2024.
Here are 5 facts about employing locum tenens clinicians that you need to know:
Locum tenens clinicians can be a short-term solution for doctor shortages, but CMOs must plan carefully how to use them.
Locum tenens physicians can plug short-term gaps in the physician workforce, but CMOs must be aware of both the cost and the effect on workplace culture.
There are about 50,000 locum tenens physicians working in the United States, says Joseph Sturdivant, MD, CMO of IMN Enterprises, a healthcare staffing company. With a clinician shortage nationwide, he notes, they're a popular solution to fill workforce gaps.
About 88% of the nation’s health systems used locum tenens clinicians in 2023, Sturdivant says, and half of them expect to use more in 2024.
"What we have seen in the rise of locum tenens is the ability to fill the void of clinicians as we have an aging population and increased utilization of inpatient care," says Sturdivant, who is a practicing locum tenens physician. "There is a lack of physician coverage throughout the nation."
Andy Anderson, MD, MBA, executive vice president and chief medical and quality officer at RWJBarnabas Health, says the health system uses locum tenens physicians in several departments.
"We have certain physician areas where we have a shortage, and having access to locum tenens physicians enables us to fill those gaps at least in the short term," he says.
Locum tenens clinicians are hired for various lengths of time, Sturdivant says. They can fill in for a week during the holidays, for a couple of months to cover maternity or paternity leave, or for several months while a healthcare organization recruits a permanent clinician.
In the longer term, Anderson says, it's more beneficial to have physicians who remain with a health system, hospital, or physician practice for long periods of time.
"Locum tenens physicians tend to come and go, and there is less opportunity for them to get to know the staff, get to know a facility, and get to know the community," he says.
Anderson says permanent clinicians are superior in the long term because they become familiar with their clinical colleagues, their institution, and the community they serve.
Financial perspective
There is a financial challenge associated with employing locum tenens clinicians, Anderson says.
"They tend to be more expensive than employed clinicians," he says. "So, in the long run financially, locum tenens is not the best model for us. It is important to fill gaps and make sure we can operate our business fully staffed. However, the incremental salary a locum tenens clinician typically demands is a cost burden."
Typically, locum tenens clinicians earn 25% to 40% more in monetary compensation than permanent clinicians, Sturdivant says. However, they are not given a benefits package as part of their compensation, which can account for one-third of the compensation that permanent clinicians have as part of their employment, he says.
Sturdivant says it's important not to view the impact in isolation.
"You must look at why organizations look at hiring locum tenens physicians," he says. "There might be a surge in patients and an organization's current staffing model cannot handle that level of patient care efficiently. Those inefficiencies can suck away the margin that serving a larger patient population can produce."
In addition, Sturdivant says, locum tenens clinicians can help to reduce doctor turnover as well as boost retention and provider satisfaction because permanent clinicians are overworked when there are openings in the permanent staff.
"If you are not meeting your staffing goals, your physicians are going to burn out and leave, which has a financial cost," he says. "When you talk about the financial bonus that locum tenens physicians receive, that cost is offset by improvements in patient care, permanent physician satisfaction, and margin that is generated from being fully staffed."
Having a pipeline to recruit permanent clinicians is an alternative to using locum tenens clinicians, Anderson says.
"In today's market, you will have a need to fill gaps here and there, but having a physician pipeline is the best solution," he says. "At RWJBarnabas, we have established a physician pipeline in partnership with Rutgers University. We are hiring physicians from Rutgers and retaining them in our communities."
Ensuring locum tenens assignments are successful
A successful locum tenens assignment, Studivant says, begins with teamwork.
"In my experience working in a locum tenens capacity, the facilities where I have struggled in my assignments are those that treated me not as a member of the team but as an expendable commodity," he says. "When I have worked as a medical director, I have had the most success with locum tenens clinicians when they are brought on as full members of the team."
Also crucial, he says, are onboarding processes.
"You want a locum tenens physician to get to know a facility and get to know the team they are working with," he says. "It is important to establish connectivity and relationships early on, so the locum tenens doctor can work as a team member with the other staff in the facility."
The onboarding process should include creating familiarity with an organization's culture, mission, vision, and values.
"They need to understand the strategic priorities of the organization," Anderson says.
That includes the quality and patient safety requirements of an organization.
"There needs to be transparency around the areas where you are focused in terms of quality and patient safety," he says. "You need to make sure that a locum tenens clinician sees the metrics that are being tracked. They need to understand the areas that are being prioritized. They also need to know how they can contribute to the outcomes that a facility is seeking."
Sturdivant says several studies have shown that locum tenens physicians compared to permanent providers are statistically indistinguishable in terms of quality care.
"[They] are not bouncing around from job to job because they are not doing a good job," he says. "They are highly educated and highly motivated professionals who have chosen to work locum tenens assignments with a skillset comparable to permanent physicians."
Sturdivant says physicians are attracted to locum tenens jobs because they can have a freedom of movement and the ability to set a working schedule.
"I personally have viewed my locum tenens work as an opportunity to put my toe in the water and test-drive different organizations and different practice patterns," he says. "Then you get the benefit of being in control. As a locum tenens clinician, you get to declare your availability in terms of scheduling."
Yale New Haven Health launched a major initiative four years ago to reduce variation in care at the health system's four acute-care hospitals and outpatient sites.
Yale New Haven Health is seeking to reduce variation in the delivery of care with the health system's Care Signature Initiative.
Decreasing variation has been a central goal of quality improvement since W. Edwards Deming pioneered the concept in the Toyota Production System in the 1970s. In care delivery, research has shown the consequences of inappropriate variation include underusing needed services, overusing unwarranted services, higher costs, and worse clinical outcomes.
Here is how Yale New Haven Health is reducing variation in care delivery.
Click here to read the accompanying article, which features comments from Thomas Balcezak, MD, MPH, chief clinical officer for Yale New Haven Health.
Clinical components of the merger between Intermountain Health and SCL Health have included integrating clinical care, integrating medical staffs, and promoting simplification of the experience of clinicians and patients.
Intermountain Health Chief Clinical Officer JP Valin, MD, MHA, has been managing the clinical elements of the 2022 merger between Intermountain Health and SCL Health.
There are several clinical aspects of the merger between the health systems. These include integrating clinical care, integrating medical staffs, and promoting simplification of the experience of clinicians and patients, Valin says in this week's HealthLeaders podcast.
When Valin came into the role as chief clinical officer of the new Intermountain Health post-merger, he was told that Rule No. 1 should be to not break anything.
"That was a great comment because both organizations had very long and storied histories of clinical excellence and providing great clinical care," he says.
JP Valin, MD, MHA, is chief clinical officer of Intermountain Health. Photo courtesy of Intermountain Health.
Over the past two years, Valin has been leading a phased approach to merging clinical care at Intermountain Health and SCL Health.
The first phase has involved "wiring and plumbing," Valin says.
"When you build a new house, you need to put the wiring and plumbing in before you can close the walls," he says. "We needed to do that work as part of our merger. We were coming from a place where both organizations did things well, but we did things differently."
For example, Intermountain Health and SCL Health had different software utilization, with one organization using MicroSoft and the other using Google.
"We had to combine on MicroSoft to be able to communicate," he says.
Intermountain Health and SCL Health have also been working to get on the same EHR. SCL Health was on Epic, and Intermountain Health used mainly Cerner. The process to shift Intermountain Health to Epic should be complete by the end of this year.
The second phase of the merger effort was a period of clinical discovery, Valin says.
"We spent time getting to know each other across the organizations and bringing together teams from the organizations to meet each other and share what each organization was doing," he says. "This second phase allowed us to identify best practices that we could share as organizations."
The third phase has involved building structures and processes to connect people together and to connect leadership structures together, Valin says.
"We wanted to align our work and integrate clinical care across the new Intermountain Health," he says. "We are more than two years into this work. We have made tremendous progress, but we are still not done."
There are better ways to retain physicians than to require them to sign noncompete contracts, the CMO of Denver Health says.
The use of noncompete contracts is widespread in healthcare, with as many as 45% of primary care physicians required to sign the agreements, according to the American Medical Association.
The FTC estimates that about 18% of the nation's workforce—roughly 30 million people—are subjected to noncompete clauses. However, in April, the Federal Trade Commission issued a final rule that banned noncompete contracts for most workers, including physicians.
The American Hospital Association and other healthcare stakeholders claim the FTC overstepped its authority to approve what the AHA calls "a bad law, bad policy, and a clear sign of an agency run amok." Now, the FTC final rule is being challenged in court.
Last month, a complaint was filed with the National Labor Relations Board that challenges a noncompete contract with part-time physicians at Mount Sinai Health System. The complaint targets a clause in the noncompete contract that states Mount Sinai part-time physicians may not recruit, solicit, or induce to terminate the employment of hospital system employees or independent contractors one year after a part-time physician's termination.
Mount Sinai declined a request from HealthLeaders to comment on the complaint.
Connie Savor Price, MD, is CMO of Denver Health. Photo courtesy of Denver Health.
"What they are probably trying to do is to prevent part-time physicians from recruiting people they have worked with at Mount Sinai," says Denver Health CMO and HealthLeaders CMO Exchange member, Connie Savor Price, MD. "This restriction bars part-time physicians from offering opportunities to colleagues at another practice or hospital."
According to Savor Price, noncompete contracts for part-time physicians are problematic for those doctors.
"For a part-time physician, noncompete contracts are particularly difficult given that they are only part-time, and the contracts limit a physician's ability to round out their employment, which should not be the purview of the employer," Savor Price says.
Denver Health does not require physicians to sign noncompete contracts.
"We don't feel the need to use noncompete contracts for physicians," Savor Price says. "We want to stay grounded in what we believe is best to service the health needs of our community. We do not see how noncompete contracts contribute to that goal."
Proponents of noncompete contracts for physicians say the agreements are helpful in retaining doctors at a health system, hospital, or physician practice.
The disadvantages of noncompete contracts outweigh the benefits, according to Savor Price, who says noncompete contracts can create a situation where a physician can be forced into working for somebody he or she does not want to work for.
"We know that workers including physicians who are not happy in their work often do not perform as optimally as they could," Savor Price says. "So, it does not serve the community to have these agreements enforced."
Satisfied physicians provide the best care for patients, according to Savor Price.
"We want doctors who want to stay here, who want to practice here, and who are happy to practice here," Savor Price says.
There are better ways to retain physicians than requiring doctors to sign noncompete contracts, according to Savor Price.
"You can provide a pleasant practice environment as well as salaries and benefits that are competitive," Savor Price says. "There are also things that can make a physician's job more interesting and purposeful. For example, many physicians like to teach, so you can provide academic opportunities."
In addition, there are different ways to compensate physicians, according to Savor Price.
"You can provide retention payments or other incentives that do not prevent a physician from going back into a community if they want to leave a job," Savor Price says.
The HealthLeaders Exchange is an exclusive, executive community for sharing ideas, solutions, and insights.
Please join the community at our LinkedIn page. To inquire about attending a HealthLeaders Exchange event and becoming a member, email us at exchange@healthleadersmedia.com.
Susan Bray-Hall, MD, was named CMO of VA Rocky Mountain Network on July 1. She had been serving as Interim CMO of the Denver-based U.S. Department of Veterans Affairs (VA) health system since November 2023. Prior to joining the VA Rocky Mountain Network, Bray-Hall served as chief of staff for the Oklahoma City VA Health Care System.
VA Rocky Mountain Network features 18,000 employees, eight hospitals, and a $5 billion operating budget. It has the largest geographic footprint of VA health systems in the lower 48 states, serving five primary states (Colorado, Montana, Oklahoma, Utah, and Wyoming) and portions of five other states (Idaho, Kansas, Nebraska, Nevada, and Texas).
One of the primary challenges of leading clinical care in such a large organization is listening and making sure that staff members are heard, according to Bray-Hall.
"I need to build relationships, spend time at all of the facilities, encourage the building of teams, and get staff to speak up," Bray-Hall says. "If I am listening to the staff, we won't miss important concerns."
For a CMO, listening is essential to promote patient safety, according to Bray-Hall.
"My primary approach to patient safety is empowering staff to speak up," Bray-Hall says. "I want staff to be able to comment on their concerns and have them taken seriously. They are the ones who are most likely to see patient safety issues."
Bray-Hall says her patient safety concerns include medication safety, surgical safety, and healthcare-associated infections, but she must be aware of the full spectrum of patient safety.
"I am concerned about taking care of patients' mental health, physical health, primary care and prevention, and all of the services in between," Bray-Hall says. "So, when it comes to patient safety for me, it is not a particular focus, it is always a global focus."
For a CMO, listening is also pivotal to promoting quality care, according to Bray-Hall.
"It is important to listen to your staff," Bray-Hall says. "The best ideas come from the frontline staff when they are taking care of the veterans."
Susan Bray-Hall, MD, is the new CMO of VA Rocky Mountain Network. Photo courtesy of VA Rocky Mountain Network.
The VA model of care
VA health systems are veteran-focused and provide comprehensive care, according to Bray-Hall.
"We embrace population health," Bray-Hall says. "We have special education for staff to care for veterans. We focus on the multi-morbid patients, so we are concerned about the global needs of our veterans. We do a ton of prevention. We provide comprehensive and coordinated care."
Given the needs of their patient population, VA health systems have several focal points, according to Bray-Hall.
"The data supports that the VA provides some of the best care in the country for cardiovascular care and preventative health," Bray-Hall says. "We are focusing on making sure that patients are getting the comprehensive care they need for their cardiovascular care in the primary care setting. Mental health and suicide prevention are core services."
Care coordination is a top priority at VA health systems, according to Bray-Hall.
"We have social workers that do care coordination and intensive case management for high-risk veterans. These are patients who have significant conditions and hospitalizations," Bray-Hall says. "We have nurses who do care coordination in primary care and that is their main job."
The VA provides care coordination in medication management.
"We have a single pharmacy record, which is extremely helpful because medications can get mixed up when a patient is going to multiple pharmacies and multiple sites of care," Bray-Hall says.
Prepared to lead
Bray-Hall is board certified in internal medicine, geriatrics, hospice, and palliative care, which provides a solid foundation to serve in the CMO role.
"I rely on my medical background all the time," Bray-Hall says. "Internal medicine gives you the breadth and knowledge base across the adult lifespan. My geriatric training taught me a lot about systems-based care and how to improve systems to provide quality care and take safer care of patients. My hospice and palliative care training taught me about listening and empathy."
Bray-Hall says her approach to leadership as CMO is to be accessible to peers and staff.
"I also share my successes and my failures," Bray-Hall says. "I want to always be authentic, which helps people feel they can come to me. I also have a connection with clinicians. I will be doing geriatric consultations via telemedicine for veterans who are frail."
Yale New Haven Health launched a major initiative four years ago to reduce variation in care at the health system's four acute-care hospitals and outpatient sites.
Yale New Haven Health is seeking to reduce variation in the delivery of care with the health system's Care Signature Initiative.
Decreasing variation has been a central goal of quality improvement since W. Edwards Deming pioneered the concept in the Toyota Production System in the 1970s. In care delivery, research has shown the consequences of inappropriate variation include underusing needed services, overusing unwarranted services, higher costs, and worse clinical outcomes.
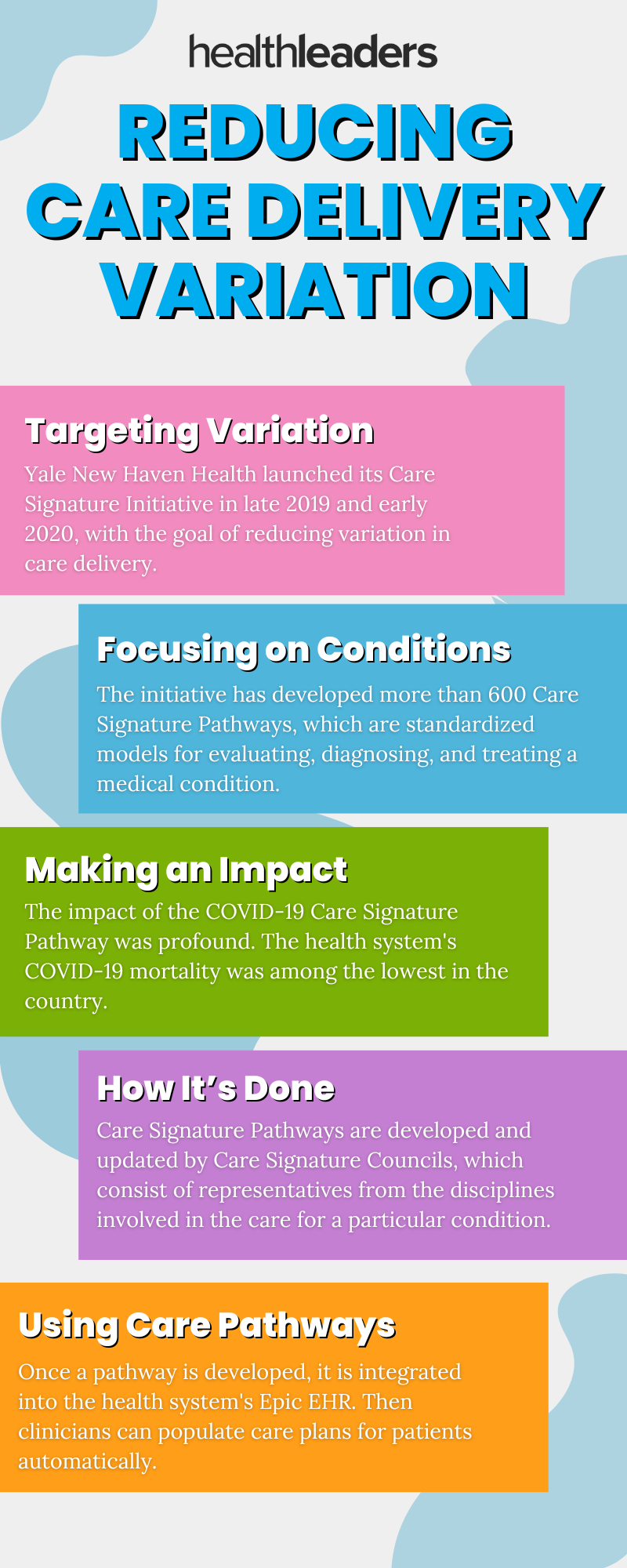
Yale New Haven Health launched its Care Signature Initiative in late 2019 and early 2020, says Chief Clinical Officer Thomas Balcezak, MD, MPH.
"The intent was based on the idea that variation is bad and that we should develop a clinical consensus on how specific conditions should be evaluated, diagnosed, and treated," he says.
The initiative has developed more than 600 Care Signature Pathways that are used thousands of times per week. The first Care Signature Pathway that the health system developed was for COVID-19, Balcezak says.
"We updated the Care Signature Pathway for COVID-19 every time a new therapy was determined to be effective, or an old therapy was determined not to be effective," he says. "As it worked out, we were updating that Care Signature Pathway practically every other day."
The impact of that pathway, Balcezak says, was profound.
"Our mortality was not only among the lowest in the country but also no different if you were in our smallest hospital in Westerly, Rhode Island, or at our academic medical center," he says. "We were able to achieve good outcomes at all of our hospitals because no matter which facility patients touched, they got the same care delivered in the same way."
Care Signature Pathways are developed by Care Signature Councils, which consist of representatives from all of the disciplines involved in the care for a particular condition. Those councils also update pathways as new medical knowledge arises.
"We give the council space and time to drive to consensus around the appropriate diagnostic work-up tests and the appropriate therapeutics for a particular medical condition," Balcezak says.
Once a pathway is developed, it is integrated into the health system's Epic EHR. Once a pathway is available on Epic, clinicians can populate care plans for patients automatically.
"We can make physicians' jobs easier by using technology to deliver recommendations," Balcezak says. "For example, if they are trying to treat pneumonia, we have a Care Signature Pathway for that condition, and they can click on a button in the EHR that populates the order set."
Thomas Balcezak, MD, MPH, is chief clinical officer of Yale New Haven Health. Photo courtesy of Yale New Haven Health.
Generating results
Balcezak says the initiative has produced positive results.
"We have gotten to a reduction in variation that has been a bedrock of quality improvement for years," he says.
For example:
Alcohol use disorder: The health system's Care Signature Pathway for alcohol use disorder recommends a treatment plan and gives the physician a recommended order set. Before Care Signature Pathways were created, only about 14% of the patients received proper treatment; now roughly 85% of patients are getting that recommended treatment.
High-sensitivity troponin test: In February 2023, a new high-sensitivity troponin test became available. Troponin is an enzyme that is released by heart tissue when it is injured, so testing for troponin in patients who present with chest pain in the emergency department can determine whether they are having a heart attack. The health system has a Care Signature Pathway for the high-sensitivity troponin test that includes the level of troponin that prompts a cardiology consult and the level of troponin that allows a patient to go home safely. The pathway has led to significant reductions in emergency department length of stay and hospital admissions.
Blood cultures: On June 28, Becton, Dickinson, and Company informed Yale New Haven Health of a shortage of blood culture bottles, forcing the health system to reduce blood culture testing. The health system created a Care Signature Pathway to address the variation in stewardship for blood cultures, including appropriate reasons to do blood cultures, appropriate intervals for blood cultures, and protocols for conducting blood cultures such as the amount of blood required. Within three days, the health system reduced blood culture utilization by 65%.
Implementing Care Signature Pathways
When a Care Signature Pathway is developed, the primary goals of the health system for introducing them to clinicians are to achieve rapid change in clinician behavior and rapidly institute standardized practice to improve operations, throughput, quality, and safety, Balcezak says.
"Each one of those factors is intimately integrated with one another," he says. "You don't get high-quality and safe care without efficient, streamlined, and standardized operations. They go hand-in-glove."
Clinician adoption has a generational element, Balcezak says.
"Clinicians have changed over time," he says. "Today's generation of clinicians is much more likely to accept suggestions and Care Signature Pathways. In the 1990s, you would hear clinicians say, 'I do not accept cookbook medicine.' Today's physicians realize that standardization is not cookbook medicine—it is best practice."
The potential to make the lives of clinicians easier is a powerful incentive for clinicians to adopt the pathways, Balcezak adds.
"Clinicians are much more likely to accept a Care Signature Pathway because it gives them answers right at the time they are seeing patients, and pathways make it easier to do the right thing and harder to do the wrong thing," he says.





 Chris Frost, MD, is senior vice president, chief medical officer, and chief quality officer at Lifepoint Health. Photo courtesy of Lifepoint Health.
Chris Frost, MD, is senior vice president, chief medical officer, and chief quality officer at Lifepoint Health. Photo courtesy of Lifepoint Health.






 JP Valin, MD, MHA, is chief clinical officer of Intermountain Health. Photo courtesy of Intermountain Health.
JP Valin, MD, MHA, is chief clinical officer of Intermountain Health. Photo courtesy of Intermountain Health. 
 Connie Savor Price, MD, is CMO of Denver Health. Photo courtesy of Denver Health.
Connie Savor Price, MD, is CMO of Denver Health. Photo courtesy of Denver Health.
 Susan Bray-Hall, MD, is the new CMO of VA Rocky Mountain Network. Photo courtesy of VA Rocky Mountain Network.
Susan Bray-Hall, MD, is the new CMO of VA Rocky Mountain Network. Photo courtesy of VA Rocky Mountain Network.
